Yemen Baseline Report
Yemen Baseline Report
Yemen Baseline Report
Mozambique WPP Baseline Report, from March 2023.
This document explores the impact of the intervention during the sixth phase of the project, which took place in the year 2020 and 2021 and focused on training women in leadership, and communication skills and equipping them with income-generating skills.
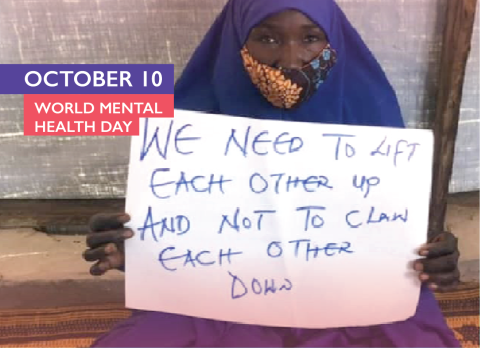
10 October 2022, Geneva– One in five persons displaced due to war or conflict will suffer from mental health problems caused by tragic events they experience somewhere in their displacement journey[1]. Unemployment, poor socioeconomic conditions, lack of social integration, and gender-based violence are risk factors for mental health conditions that are more likely to affect displaced women than men[2].
On World Mental Health Day, we explore how the Women's Participation Project (WPP) supported displaced women and girls' psychological well-being by attuning their voices, addressing their needs, promoting gender equality, and encouraging economic independence, as these values have proven a direct and beneficial effect on women's mental health [3].
"The project has equipped me with different skills that have made me look at myself with more confidence and strength. I am more aware of my worthiness, power and resilience as a woman, mother, and community member. " a female survivor of Ecuador's earthquake mentioned.
The Project has supported women in knowing their rights and participating in decision-making in the sites: "Before participating in this project, I was confined in a room, weeping all day. Then I decided to be proactive and part of a women's committee. After receiving the leadership training, I feel I can do many things, explain many issues, and help other women address their needs." said a displaced woman living in Bangladesh.
The lack of information about food distribution or how to obtain essential services could trigger humanitarian response-induced anxiety [4]. The WPP allows women equal access to information and services and provides awareness sessions on different topics: "I can now help protect my family and community from COVID-19 after the awareness training I received. Women are reaching out to me to learn how to make masks, which makes me feel valued in my community." A displaced woman from South Sudan said.
The initiative supported women to learn new skills and engage in breadwinning activities leading to economic independence and personal satisfaction. "I learned how to tailor and make bedsheets and tablecloths. Now I am earning a steady income and contributing to my family, and I feel so proud of this achievement ". Another woman from South Sudan stated.
The project has also educated men on women's rights and stimulated change by letting them experience the difficulties women and girls face due to gender: "Our society favours men over women, and this must change now; as we leave this training, we should be the change-makers in our society," said one male training participant in South Sudan.
The Women's Participation Project, a global initiative implemented by IOM, will continue to support equitable and meaningful participation and representation of displaced women and girls. Initiated in 2016, the project is a part of the 'Safe from the Start' Initiative funded by the Bureau of Population, Refugees, and Migration (BPRM).
The project has helped amplify the voices of more than 5000 displaced women and girls in 12 countries worldwide and has contributed to mitigating the risk of gender-based violence in these locations.
References:
[1] https://www.who.int/news-room/fact-sheets/detail/mental-health-in-emergencies
[2] https://www.who.int/news-room/fact-sheets/detail/mental-health-in-emergencies
[3] https://www.un.org/womenwatch/daw/csw/mental.ht
[4] https://www.who.int/news-room/fact-sheets/detail/mental-health-in-emergencies
Victoria finds life in the Naivasha camp extremely dangerous. As women and girls lack access to education and economic opportunities, it is challenging to be financially independent or feel confident to be engaged in breadwinning activities.
"Often men let off steam on their wives because they are unemployed and unable to carry the burden of providing for their families alone," Victoria says. She also adds that women do not only face gender-based violence in their homes but are also subject to harassment and rape from men on the site.
Under the Women's Participation Project implemented by IOM in South Sudan, Victoria has learned to tailor and sell bedsheets and tablecloths and has received leadership training that helped her boost her self-esteem. The Project aims to enhance livelihood opportunities and strengthen participation for displaced women and girls, mitigating the risk of gender-based violence.
"With the revenue I am earning as a tailor, I was able to send my three children to school and participate in the household's expenses," Victoria announces proudly.
With the support and leadership training Victoria received throughout the Project, Victoria could identify the needs of displaced women and girls on the site and address solutions to their problems: "Displaced young girls require education and vocational training in tailoring, bread making, protection and job opportunities to support their lives and families."
Victoria recognises the difference she could make as an empowered young woman who can provide for herself and her family. This realisation had made her self-confident and ambitious: "In five years, I see myself working in an NGO or a government institution, living outside of this camp, raising my kids in a better house and sending them to better schools."
The Women's Participation Project that supported Victoria and others derives from a global initiative implemented by IOM and other organisations in different displacement contexts and settings to support equitable and meaningful participation and representation of displaced women and girls. Initiated in 2016, the WPP is part of the 'Safe from the Start' Initiative funded by the Bureau of Population, Refugees, and Migration (BPRM).
The WPP Project has helped amplify the voices of more than 6000 displaced women and girls in 12 countries worldwide and has contributed to mitigating the risk of gender-based violence in these locations.

On 31 October 2000, the UN Security Council adopted Resolution 1325 emphasising the role of women in the prevention and resolution of conflicts and calling for equal participation of women in peacebuilding efforts. Twenty years down the line, women still remain the minority around negotiation tables and in peacebuilding operations, with their specific needs in conflict situations often being overlooked.
Yet they often represent a significant share of all conflict-affected people: at the end of 2019, nearly 23 million women and girls worldwide were living in internal displacement because of conflict or violence. To make real progress, we not only have to fully include women at all levels of security and peace operations, but also better address the needs of (internally) displaced women and girls.
Even though studies suggest that women’s participation in conflict prevention and resolution can improve outcomes, women are still frequently excluded from formal peace negotiations. Research by the Council on Foreign Relations shows that, between 1992 and 2019, women, on average, only constituted 13 per cent of negotiators, 6 per cent of mediators and 6 per cent of signatories in major peace processes. The year 2020 has so far confirmed this trend: women represented only around 10 per cent of negotiators in the Afghan peace talks, just 20 per cent of negotiators in Libya’s political discussions (no women took part in the military talks) and 0 per cent of negotiators in Yemen’s peace process. As for UN peacekeeping operations, in 2020 women made up only 4.8 per cent of military and 10.9 per cent of police personnel.
While the statistics mentioned above surely have to change to ensure equal participation of women – something that has also been clearly acknowledged by the United Nations – efforts to build sustainable peace will need to go beyond these numbers. Johan Galtung, one of the founders of peace and conflict studies, distinguishes between negative and positive peace. While the former is defined by the absence of direct or personal violence, such as war, assault and terrorism, the latter includes the absence of indirect or structural violence, such as social injustice, poverty and hunger. Working towards positive peace, therefore, requires us to look at the bigger societal picture, including the living conditions of civilians affected by conflict and war.
In the context of Resolution 1325 this means, among other elements, taking into account the specific vulnerabilities of women and girls displaced as a result of violence and war. Already 20 years ago, women and children in internal displacement were mentioned as one of the groups particularly at risk in the resolution’s preambulatory clauses. Today, this is backed up by evidence showing that women are overall more severely affected by displacement than men.
Recent studies and research from around the world compiled by IDMC demonstrate how displacement is taking a disproportionate toll on women’s livelihoods, security as well as access to health services and education. A study in Ethiopia’s Oromia region showed that 35 per cent of surveyed women became unemployed as a result of their displacement, compared with 30 per cent of men. Research in Somalia found that school attendance increased for displaced boys from 29 to 41 per cent, while it decreased for displaced girls from 45 to 29 per cent. Studies in Colombia and Afghanistan point to an increase of domestic violence following displacement. Surveys conducted in Somalia and Ethiopia show that more women than men felt their physical health had deteriorated since their displacement.
If the above-mentioned impacts of internal displacement on women and girls are not addressed, they have the potential to reinforce each other in a vicious circle of vulnerability. Girls’ low school attendance rates may constrain their mothers’ ability to engage in work because they have to stay at home to care for them. Mothers’ lack of opportunity to establish a decent livelihood will in turn make them less able to afford to send their children to school or provide for health care, and stress due to insufficient funds might increase domestic violence.
On a more positive note, taking into account the specific needs of internally displaced women and girls can greatly contribute to breaking the vicious circle and creating what Galtung called positive peace. Ensuring displaced women and girls are fully involved in decision making and can benefit from tailored humanitarian and development support, backed by robust legal and policy frameworks, is essential to guarantee responses that bring about lasting peace. Focusing on women and girls could go a long way towards achieving durable solutions and fostering socioeconomic development for all.
Only if we manage to achieve both, putting an end to hostilities through the full inclusion of women in negotiation and peacebuilding processes, and constructing post-conflict societies with equal opportunities for all, can we realise the full potential of UN Security Council Resolution 1325. Twenty years after its adoption, it is about time.
This article is part of a new IDMC series of policy blogs. In the coming months we will periodically reflect on significant policy developments through an internal displacement lens.
Read the full article here!

COVID-19 has upended the lives of children and families across the globe and is impacting efforts to end child marriage and female genital mutilation (FGM). This technical note compiles some of the evidence on harmful practices in the time of a public health emergency and proposes programmatic responses on a policy level; systems level; in terms of evidence and data; and on the level of communities and individuals.
Read the full note by UNICEF here!
In line with our strategic commitment to target the most pressing challenges in the sector and to ensure that innovation processes are evidence-based and problem-led, we commission robust gap analyses.
Since 2015, we have dedicated resources, focus and support to innovation that tackles the complex and egregious problem of gender-based-violence (GBV) in humanitarian settings. We have worked collaboratively with, and been guided by, key agencies and experts within the GBV in emergencies community. In 2016, we published our first-ever GBV Gap Analysis in which key challenges across this sector were identified, evidenced and prioritised, and then transformed into opportunities for innovation.
We are now sharing with the sector our second Gap Analysis focused on GBV humanitarian settings which seeks to update the outstanding and persistent gaps that continue to challenge the GBV sector. It builds upon our first Gap Analysis, providing a further breakdown of how challenges, such as the need for quality GBV expertise or improved monitoring and evaluation of GBV programming, manifest across different types of GBV programming. With this adaptation, we aim to present a wider breadth of gaps experienced across humanitarian GBV efforts and to increase the relevance of this report for more actors, such as non-GBV actors working to mitigate risks of GBV.
Similar to the first Gap Analysis, this report identifies both operational and systemic challenges faced by the sector, continually acknowledging the complexity and diversity of needs across the sector in order to achieve its intended positive outcomes for women and girls in humanitarian settings.
Read the full report by ELRHA here!
In a matter of months, the swift spread of the novel coronavirus has had devastating ramifications on global public health. As of May 1, 2020, there were more than 3.3 million confirmed cases of COVID-19 around the world. In addition, the pandemic is having tremendous effects on the economy and social fabric of every society.
Since the outbreak began, humanitarian workers, journalists, and researchers have warned that people in displaced communities are at high risk for contracting and spreading the virus. Globally, approximately 71 million people—or one out of every 108 people—are forcibly displaced. A majority of them live in countries with weak and under-resourced healthcare infrastructure where systems are unlikely to be capable of handling the scale of this crisis. Even in some of the wealthiest countries such as the United States, COVID-19 is exposing massive gaps in the healthcare system and significant inequalities resulting in deadly outcomes.
Displaced persons—including refugees, asylum seekers, internally displaced people (IDPs), and stateless people—often live in especially cramped quarters, have limited access to health services, are not included in public information campaigns, work in the informal economy, and face restrictions on their movement. These conditions create significant challenges even when there is no global health emergency. In the context of a pandemic, however, they become more acute, increasing the risk of individuals contracting and spreading the disease. Moreover, the additional strain on governmental and non-governmental organizations’ (NGO) finances as a result of the current health crisis is likely to further stretch the humanitarian system and exacerbate displaced communities’ difficulty accessing basic needs and staying safe.
Within already vulnerable displaced communities, women and girls are at even greater risk. Cultural norms, underrepresentation, and a host of other challenges further marginalize them socially, politically, and economically. As a result, forced displacement uniquely and disproportionately affects women and girls, as does this pandemic. Recognizing their particular circumstances “is a fundamental step to understanding the primary and secondary effects of [this] health emergency on [women and girls], and for creating effective, equitable policies and interventions.”
This pandemic has an outsized impact on women and girls and augments existing vulnerabilities. This impact should inform decision-making related to preventing and responding to the disease’s spread. Local and national government officials, humanitarian actors, donors, community leaders, and medical professionals each have roles to play in managing the outbreak and its varied effects on all aspects of society. These actors need to urgently analyze the gendered impacts of COVID-19 in displacement to mitigate the negative ramifications for displaced women and girls. As the UN High Commissioner for Refugees Filippo Grandi notes, “what this global coronavirus outbreak has undeniably demonstrated, is that the health of every person is linked to the health of the most marginalized and vulnerable members in a society.”
Livelihoods and Education
Worldwide, women perform three times more unpaid caregiving work than do men, accounting for 76.2 percent of the total hours worked. Refugee and other displaced women do not escape this trend—social norms often dictate that they take care of children and elderly family members and manage the household. Those responsibilities increase as people become sick, putting women and girls at heightened risk of becoming infected during a health crisis. The added responsibilities at home also undermine women’s and girls’ economically productive opportunities, as evidenced during the Ebola outbreak that began in 2014.
For example, girls have more difficulty accessing education, including alternative means like homeschooling. For women, it becomes more difficult to engage in remunerative activity. However, having a source of income is critical for refugee women, at least 25 percent of whom are heads of their households. International aid is rarely sufficient to meet families’ basic needs: many refugees living in urban settings might not receive any outside assistance at all. Further complicating the ability of refugees to earn an income, host country governments often bar refugees—especially women—from the formal labor market. For Syrian refugee women across Lebanon, Turkey, and Jordan, for example, becoming a wage earner is both a new and essential opportunity.
However, in taking difficult steps to prevent the spread of the coronavirus, governments around the world have ordered both formal and informal workplaces to close. As a result, livelihood opportunities that were already scarce and difficult for refugee women to access are even less attainable. Even after the health crisis abates and governments lift lockdowns, the immense and as yet unpredictable economic damage from the COVID-19 pandemic will have lasting repercussions for refugees’ ability to access work.
Economic uncertainty, in turn, further hinders girls’ access to education. Families facing economic hardship—particularly those living in low-income countries—must weigh the financial and opportunity costs of sending their children to school rather than to work or help at home. Due to the prevailing gender norms in many societies, girls are often the ones to lose out. In families whose economic difficulties are exacerbated by displacement, parents may choose not to educate their daughters. Indeed, refugee girls are only half as likely to enroll at the secondary level as boys.
Authorities’ decisions to close schools in order to prevent the spread of the coronavirus—albeit important to protect public health—are therefore likely to have lasting negative consequences for girls. Once girls are taken out of school for any reason, they are both less likely than boys to engage in homeschooling and less likely to ever re-enroll. By forcing schools to close, the pandemic thus threatens the education of the more than 740 million girls who are enrolled but are currently not attending due to COVID-19 related closures.
A lack of financial security and the related lack of educational opportunities are also directly linked to an increase in women’s and girls’ reliance on negative coping mechanisms and the risk of exploitation. These risks—including transactional sex, forced and early marriage, sexual abuse, and human trafficking—are also greater for women and girls who are forcibly displaced. For example, in several Latin American countries hosting Venezuelan refugees and migrants, Refugees International found that displaced women and girls who lacked economic or educational opportunities were at higher risk of sexual exploitation. This is true of other displaced populations, as well.
Ensuring that women and girls have adequate educational and livelihood opportunities is thus critical to mitigate the harmful effects of financial insecurity. However, as the COVID-19 pandemic ravages economies throughout the world, refugee-hosting countries—the top four of which are Turkey, Pakistan, Uganda, and Sudan—will struggle to provide such opportunities even for their own citizens. It is unlikely that refugee women will be a priority, despite research indicating that refugees’ access to the labor market generates more benefits than costs.
Access to Health Services
Inadequate access to even basic health services has long been a challenge for millions of forcibly displaced people. National healthcare systems of host countries typically exclude refugees while IDPs in conflict-affected countries struggle because health infrastructure may be damaged or destroyed. In Syria where more than 6 million IDPs reside, systematic and targeted attacks on health infrastructure as well as restricted aid into areas like Idlib, make identification of the coronavirus and adequate treatment for those infected nearly impossible. For women and girls, these limits to accessing health services have particularly severe consequences.
Women and girls have unique healthcare needs that are crucial to their safety and well-being. However, as governments, donors, and aid providers redirect most of their attention and resources toward COVID-19 prevention and response, it is leaving women and girls unable to obtain other vital medical care to which they consistently need access. Sexual and reproductive health services (SRHS)—which are already insufficiently available for many displaced individuals—are being interrupted or eliminated altogether. Without adequate family planning services, unplanned pregnancies will increase and, in turn, increase the importance of adequate maternal healthcare.
Globally, 61 percent of maternal deaths occur in fragile states, including ones affected by conflict and natural disasters where many refugees and IDPs live. Humanitarian aid providers’ experiences in past public health emergencies have demonstrated the importance of maintaining uninterrupted access to maternal health care—including prenatal and neonatal care—for displaced women during crises. For example, the closure of maternal health clinics in West Africa during the Ebola crisis resulted in a 70 percent increase in the region’s already high maternal mortality rate. In Sierra Leone alone, disrupted maternal health services and fear of seeking treatment due to the outbreak, contributed to about 3,600 maternal deaths, neonatal deaths, and stillbirths. This number rivals the number of deaths in the country from Ebola itself.
Prioritizing maternal health is especially important because studies show that “pregnant refugee women show higher rates of adverse pregnancy outcomes, including caesarean section, stillbirth, and other maternal and perinatal morbidities.” Thus, while public health officials must dedicate adequate resources to protect both men and women from COVID-19, they must also continue investing in the health of mothers and newborn children. Additionally, while medical professionals do not believe pregnant women have a higher risk of contracting the disease than other adults, according to the U.S. Centers for Disease Control (CDC), pregnant women “have had a higher risk of severe illness when infected with viruses from the same family as COVID-19 and other viral respiratory infections, such as influenza.” Thus, once infected, pregnant women may have a higher risk of developing complications from the disease.
Protecting their health means also recognizing that simply going to the hospital to give birth might increase a woman’s risk of contracting COVID-19. Indeed, at the end of March 2020, a new mother became the first refugee to test positive for COVID-19 in Greece, and reports suggest she could have been exposed when she delivered at the public hospital. The CDC also recommends that “pregnant people should protect themselves from COVID-19 avoid people who are sick or who have been exposed to the virus.”
Pregnant women should not be left to weigh the benefits of going to a hospital against the risks of exposure to the virus. They must have access to safe healthcare facilities where they are confident that medical professionals are taking the necessary precautions to limit the exposure women giving birth have to other patients. Although the challenges are typically greater in displaced communities where healthcare facilities are often extremely limited and under-resourced, medical professionals should designate separate areas for patients being treated for COVID-19 so as to keep pregnant women safe.
Water, Sanitation, and Hygiene (WASH)
Good hygiene practices, such as frequent handwashing, and adequate water and sanitation services are essential to prevent COVID-19 and break the chain of transmission. According to the UN Refugee Agency (UNHCR) technical WASH guidance, “WASH practitioners should work to enable more frequent and regular hand hygiene by increasing access to soap, increasing access to handwashing facilities, and using proven behavior change techniques.”
However, complying with these recommendations is difficult for forcibly displaced people who often live in crowded camps or urban areas. Cooking, bathing, and bathroom facilities are often shared or inaccessible. In camps hosting asylum seekers on the Greek islands, there is one latrine for every 160 people and one water tap for every 1,300 residents. In a settlement hosting South Sudanese refugees in Uganda, just over half of the refugees have access to latrines at all.
Even if there are bathroom facilities, women and girls might not feel safe using them. This is true in the Greek camps described, where Refugees International found that most women and girls feared using a latrine or one of the few water taps where handwashing was possible. Women and girls in these camps explained that because the police force is virtually non-existent and some latrines do not have lights or locks, they were at risk of being harassed or attacked when using them. In fact, such insecurity is so widespread and acute among displaced populations that the U.S. Congress introduced the 2019 Refugee Sanitation Facility Act. The bill requires humanitarian organizations receiving U.S. government funding to provide locks and well-lit pathways to facilities.
Once again, women and girls cannot be left to choose between their personal wellbeing and exposure to COVID-19. Governments and humanitarian organizations must take steps to make it possible for displaced women and girls to follow health officials’ instructions. This must include increasing the number of safely accessible sex-segregated latrines and handwashing stations in camps and settlements where asylum seekers, refugees, and IDPs live. In urban settings, it is important to know where displaced people access water and bathroom facilities and to what extent women and girls have difficulty accessing these facilities. Humanitarian actors and government officials should conduct up to date mapping of these of these communities. They should also conduct rapid safety audits of these areas. This type of audit looks at the extent to which the physical layout of a community potentially makes women and girls more or less vulnerable to threats of GBV. Where women feel unsafe or that they cannot easily access water, bathrooms, and soap, humanitarian actors and local governments must urgently work together to improve the water supply and provide soap as needed.
Providing for displaced women and girls during the coronavirus pandemic must also include ensuring access to menstrual hygiene and sanitary materials. As in other times of crisis, decreased household income, and the resulting competition for resources may make these materials unaffordable. Moreover, the supplies—including sanitary pads, underwear, and soap—may also become unavailable to women and girls who rely on humanitarian agencies for them. Worldwide, the response to the coronavirus has resulted in reduced funding for humanitarian operations not directly related to the pandemic; border closures and lockdowns that affect global supply chains; and travel restrictions that limit humanitarian aid workers’ access to displaced communities.
A recent survey of residents in the Azraq refugee camp in Jordan, which has been under lockdown since March 21, 2020, found that obtaining WASH materials, including feminine hygiene products, was the second most urgent priority for refugees. Humanitarian responders must take added measures to ensure that girls and young women who are homebound or are cut off from humanitarian aid still can access safe distribution of dignity/hygiene kits and contraceptives. Together with healthcare workers, humanitarian aid agencies should not only provide feminine hygiene materials—including to infected women and girls who are in isolation or treatment centers—but also provide safe and private areas to dispose of these materials.
Gender-Based Violence (GBV)
Already ubiquitous in societies worldwide, gender-based violence (GBV) becomes even more likely during crises, when family and community protections are disrupted. Such is the case during the coronavirus pandemic. While GBV can affect men and boys, GBV primarily affects women and girls as well as LGBTI individuals. It is a life-threatening health and human rights issue that is exacerbated in emergencies, including in the context of displacement.
One of the most common forms of GBV is intimate partner violence (IPV) or domestic violence—violence perpetrated within one’s own home or family. For refugees and other forcibly displaced people, IPV is usually the most pervasive form of GBV and one that escalates rapidly without checks in place. Researchers have documented this in a variety of settings including Iraq, Kenya, and South Sudan.
Factors that lead to such high levels of IPV in forcibly displaced communities include “rapidly changing gender norms triggered by displacement, women’s separation from their parents and families, forced marriage and re-marriage, poverty, and male substance use.” As Refugees International’s recent research documented among IDPs in South Sudan, a country with high levels of conflict-related sexual violence (CRSV) perpetrated by armed actors, there, “the biggest risk for women is still within the household.” As a result, the “stay at home” orders that governments in most countries have imposed to reduce the spread of the coronavirus create significant risks for women and girls.
As part of the response to the pandemic, government officials have subjected more than a third of the world’s population to movement restrictions across and within countries, including mandatory mass quarantines and border closures. These measures, while helping to slow the spread of the disease, are also causing an alarming spike in the levels of IPV. In April 2020, UN Secretary-General, António Guterres noted that there had been a “horrifying global surge in domestic violence” as a direct result of lockdowns due to the COVID-19 pandemic. Within just a month of the World Health Organization (WHO) declaring the coronavirus a pandemic, China, Italy, Turkey, Brazil, Spain, France, the United Kingdom (UK), and Greece reported that domestic violence cases among women had risen dramatically, as women have been quarantined with abusers.
Similar trends are likely to be seen among displaced populations. NGOs operating in the Rohingya refugee camps in Bangladesh are already seeing higher rates of IPV than usual. The Gender in Humanitarian Action Working Group (GIHA WG) in Cox’s Bazar highlighted this issue in a recent statement, “Preliminary indications suggest an increase in the number of GBV cases particularly intimate partner violence and child marriage.” These preliminary rates of IPV likely undercount the reality because mobile network restrictions in the camps and reduced numbers of humanitarian staff make reporting difficult. As tensions in households increase and already sparse community structures are further weakened by movement restrictions and social distancing directives, rates of IPV will inevitably continue to rise in Cox’s Bazar and in other displaced communities.
At the same time as incidents of GBV such as IPV increase, services for survivors are often not readily available. Indeed, there is typically little funding available for GBV-related programs in the response to humanitarian crises. Between 2016 and 2018, donors and aid organizations allocated only 0.12 percent of all humanitarian funding to GBV prevention, mitigation, and response activities. This is true despite the United Nations Population Fund’s (UNFPA) assertion that “violence against women and girls is one of the most prevalent human rights violations in the world.”
If the preliminary data are correct, some quarantine measures designed to slow the spread of the COVID-19 are heightening the risk of GBV for women and girls. Therefore, it is essential that donors boost the levels of GBV-specific funding to levels commensurate to the scale of the problem. UN agencies have recently asked donor states to provide $2.012 billion of additional support for all coronavirus related activities through the coordinated, Global Humanitarian Response Plan (HRP) for COVID-19. The HRP requests a combined $375 million for UNHCR—the agency responsible for forcibly displaced people, and UNFPA—the agency responsible for women’s health. This funding is for all COVID-19 related activities. It is also inclusive of any supplementary provisions to prevent and respond to GBV and to maintain consistent access to women’s specific healthcare through December 2020.
Prior to this pandemic, external studies demonstrated that donors and aid organizations only provided one-third of the funds required for GBV risk mitigation and response interventions to meet basic standards of care. Thus it is imperative that donors and humanitarian organizations increase the percentage of money they allocate to GBV programming at least threefold. But they must go even further. It is also essential that they quickly surge extra funds to address the additional increase in GBV due to COVID-19.
GBV service providers have always been crucial in providing treatment and support for victims of IPV and other forms of violence in displaced communities. As some of the organizations that specialize in these services are forced to discontinue or disrupt services because of the pandemic—due to restrictions and/or funding constraints—it is vital that the organizations update GBV referral pathways to reflect changes in available care facilities. Community leaders and other relevant organizations need to be informed about those updated pathways.
Information Sharing and Leadership
Displaced populations often face obstacles to accessing information and exclusion from decision-making that directly impacts them. Typically, women and girls are even further marginalized. They are denied leadership roles within their communities, while their domestic caregiving responsibilities prevent them from attending public information sessions. Additionally, a lack of language skills and illiteracy can further isolate them from important information sharing and outreach activities.
Access to accurate, up-to-date, and relevant information is essential to protecting individuals and communities from the coronavirus. To decrease the risk of infection, as well as mitigate stress and other protection risks, government-led, public health information campaigns must include displaced people and take specific measures to reach women.
Humanitarian workers providing information about COVID-19 should use tactics that take into account differences between men’s and women’s literacy rates, access to mobile phones, and ability to participate in outreach activities. During the Ebola crisis, for example, public health officials in Nigeria shared crucial messages about the disease via radio and television for women who were unable to read written health notices. Learning from these past emergencies, government and NGO efforts must tailor their methods of communication to the context, ensuring they will effectively engage women.
Even as many displaced women and girls have limited access to information, some women act as powerful community leaders or as part of strong formal and informal community networks. These roles give them considerable influence. Research shows that during the Ebola crisis, although government officials controlled decisions about school closures and movement restrictions, the community leaders largely determined what people knew about the disease, whether or not they trusted the information provided, and how they responded.
In dozens of displacement settings both urban and rural, international aid organizations train Community Health Workers (CHW) to act as liaisons between the organizations and displaced people. These CHW provide those in their communities with information about available services, encourage them to seek out those services, and carry out awareness- raising and educational campaigns. International organizations have utilized CHW among displaced Syrian communities to successfully mitigate measles outbreaks. NGOs can adapt this model—in which they empower community members to communicate with their peers and share information—to the current COVID-19 pandemic.
Although both men and women can serve as CHW, aid organizations and government officials should prioritize elevating female CHW to better reach and build trust with women in displaced communities. A female Congolese refugee and former CHW in Tanzania is now the elected chairperson of a 150,000-person refugee camp and is an important example of how supporting women’s leadership can be extremely valuable. Public health officials and humanitarian organizations should capitalize on the trust that these women have with members of the community and empower them to share life-saving information related to COVID-19.
Targeted Data Collection
To understand how COVID-19 and its repercussions affect displaced women and girls differently than men and boys, accurate data must be available. However, getting that data is a challenge. The disease is moving rapidly and the capacity to collect reliable data varies widely across affected countries and communities. Further, most governments have not viewed testing, surveillance, treatment, and data collection in displaced communities as a high priority.
Lebanon, for example—where more than 1.5 million Syrian refugees reside—has not proactively made an effort to test refugees for the disease. Even if refugees exhibit symptoms of COVID-19, the many whose legal papers are outdated may avoid testing for fear of being deported to Syria. Although UNHCR is working with the government to ensure refugees do not face legal consequences if they seek testing, such fears are unsurprising—upwards of 70 percent of Syrian refugees in Lebanon lack residence permits and the Lebanese government forcibly returned more than 2,500 Syrians in 2019.
Where governments, public health officials, and medical professional collect data about COVID-19 testing and treatment, they should immediately disaggregate the information by sex and, ideally, by age and pregnancy status, as well. These government and health professionals should make the data publicly available to inform decisions about providing aid and health services to communities in need while upholding confidentiality and privacy protections.
It is too early to fully predict how the COVID-19 pandemic will affect people differently according to their gender. However, the outcomes of the recent Ebola and Zika epidemics clearly show that during public health emergencies, gender matters. Gender, in particular, is a strong determinant of an individual’s economic stability, access to health, vulnerability to violence, access to information, and overall quality of life. This is especially true for displaced communities.
Recommendations
Governments where IDPs, asylum seekers, refugees, and stateless people reside should:
Disaggregate COVID-19 related data by sex, age, and pregnancy status and immediately make it publicly available, while also ensuring an appropriate level of data privacy and confidentiality. In contexts where the capacity for data collection is low, provide urgent technical capacity building by seeking assistance from other countries, especially those that have passed through the worst of the pandemic. Use this data to conduct a rapid gender analysis when making decisions about funding, service provision, and public health orders impacting forcibly displaced people.
Prioritize investments in and the creation of livelihood opportunities for displaced women, such as home-based businesses that can deliver products or services within quarantined communities, allowing women to earn money even as they take on additional caregiving responsibilities. Provide loans and cash assistance grants in areas where markets are still functioning. As movement restrictions are lifted, facilitate access to the formal and informal labor market economies for displaced people including women, by ensuring that they have the legal right to work and can register their businesses.
International organizations, NGOs, and donors working with forcibly displaced populations should:
Prepare for an increase in intimate partner violence (IPV), transactional sex, forced and early marriage, sexual abuse, and human trafficking among displaced women and girls by ensuring uninterrupted access to sexual and reproductive health services (SRHS), contraceptives, and gender-based violence (GBV) prevention and response services. In case of disruption of GBV service provision, update referral pathways to reflect changes in available care facilities, and inform relevant actors about those changes.
Provide adequate maternal health care and regular provision of menstrual hygiene materials to women and girls of reproductive age in displaced communities. Take extra precautions to ensure pregnant women can safely give birth without being exposed to the coronavirus. Do so by financially supporting health clinics and hospitals so that they can remain open and encourage them to treat COVID-19 patients separately than mothers giving birth.
Build in budget lines specifically for programming focusing on and responding to the exploitation of women and girls and their health in all COVID-19 related appeals and programming. Ensure close monitoring and accountability of these funds through regular reporting. Do not divert funding already allocated for specific and ongoing health needs of women and girls to COVID-19 related health services.
Increase safe access to clean water, latrines, and handwashing facilities by installing more sex-segregated latrines and handwashing facilities equipped with locks and lighting in camp settings. In urban settings, conduct rapid mapping exercises to better understand access to personal hygiene in areas where displaced people are located. Simultaneously, conduct basic safety audits to assess the risks women and girls face when adhering to basic health protocol such as frequent handwashing. When taking measures to respond to COVID-19, use the information from the mapping exercises and safety audits to improve women’s and girls’ safe access to WASH facilities.
Include displaced people, especially women and girls, in public health information campaigns, testing, and other services. Include all displaced people, especially women and girls, in public health information campaigns, testing, and other services. Ensure that this information sharing is accessible and understandable. Use several forms of communication including written materials, visual graphics, radio and TV to establish a wider reach, given the higher levels of illiteracy among women. When sharing information through mobile phones and other devices, ensure that women and girls have access to mobile phones and the internet.
Capitalize on the trust that female-driven community networks have, by training more women as Community Health Workers (CHW) and set aside funding to compensate them. Empower these women to complement the work of medical health professionals, by encouraging them to share life-saving public health information related to COVID-19 within their communities.
Read the full article here!

As part of NORCAP's Accelerator Program, our five female junior energy experts are pushing for a clean energy transition. To them, women are the most important pieces of the puzzle.
"In many African communities, women and girls have the main responsibility for collecting firewood. While walking considerable distances from their homes, they are often subjected to sexual harassment and rape. When we provide these women with other, more effective energy solutions, the impact is immense", says energy expert Purity Kendi, who is currently deployed to UN Refugee Agency (UNHCR) in Tanzania.
Purity is one of the five junior energy experts participating in NORCAP’s Female Accelerator Program, a project that was launched last year, aiming to increase female participation and build capacity within the renewable energy sector.
"Women contribute to the entire energy value chain. If we are to succeed with the clean energy shift, women and girls have to be included from the start", Purity says.
A shift to renewables is pressing, and not just in order to reduce global warming. Transitioning to cleaner, more efficient energy solutions such as solar power, biogas, briquettes or more efficient cooking stoves can have wide ranging implications for daily lives in refugee and host communities.
Hazardous indoor air from firewood stoves and diesel generators is a huge global health problem, causing respiratory disease in women and children especially. Not having access to light makes it difficult for children to do their homework, as well as restricting opening hours for shops and other businesses and rendering streets dark and unsafe.
In addition, there is the previously mentioned perilous wood collecting, which can require spending as much as 10 to 15 hours per week.
"Energy influences everything, from cooking to food storage, water access, health care and livelihood opportunities. In the humanitarian community, energy is not even recognized as a cluster of its own. It's cutting across the whole humanitarian response", says Anaïs Matthey-Junod, who is currently working with International Organization for Migration in Switzerland.
Anne Nyambane is deployed to the Food and Agriculture Association in Uganda, working on projects such as building farmer schools powered by solar energy and developing briquettes made of biowaste.
As a young girl, she used to dream of modernising her parents’ lives in their village. One of the things she wanted to do, was to make her mother’s cooking experience cleaner and easier, away from the smokey three stone fire.
A few years ago, she built her mother a modern kitchen and installed a stand-alone LPG and electric gas cooker. When she visited her parents during the Christmas period, however, Anne was surprised to see the cooker looking brand new.
"When I asked her why she wasn’t using it, my mother said that she preferred to sit while cooking. Also, the new cooker could not hold the pot in place when stirring the food, which frustrated her. My intention was good, but the urban technology I had offered her just wasn’t appropriate".
This lesson is something Anne brings with her into the field, where she frequently approaches women for informal conversations.
"When speaking to them, I make mental notes instead of writing. In that way, they don’t feel like they are being interviewed, and the information I get is often very legit and raw. In many cases, that gives me an idea on what my next project should be", she says.
One of the ways in which the five energy experts believe they can contribute to better clean energy solutions, is just that: Their ability to reach women, and especially in communities where women are more or less restricted from speaking with men.
"While women occupy a fundamental role in the use of household energy, the question of which energy solutions to acquire is often taken by men. In some cases, the given gender or social norms might mean that female humanitarian workers are best placed to help women’s voices get heard and help meet their needs", says Rebeca Solis, who is deployed to World Food Programme in Italy.
![]()
"I get great satisfaction from knowing that what I am working on will make a difference in people's lives, improving their energy access and well-being", says NORCAP energy expert Nour Al Najjar. Here she is pictured on a recent energy assessment mission for the Norwegian Refugee Council in the Azraq refugee camp in Jordan. (Photo: NRC)
Nour Al Najjar, who is currently working on solarising schools, shelters, and camps with the Norwegian Refugee Council in Amman, Jordan, agrees.
"Without the involvement of women, who are users and, in many cases, producers of energy, projects risk being ineffective. And when the energy projects aren’t representative of actual needs, they will fail to provide adequate solutions for the entire targeted community", she says.
Despite the strong linkages between gender and energy, women far from abound in the field of energy. According to the International Renewable Energy Agency, renewable energy employs about 32 percent women, compared to 22 percent in the overall energy sector.
"I think the imbalance has to do with gender stereotypes, for example that women are underrepresented in STEM subjects. There is also the misconception that you have to be an engineer to be an energy expert", says Anaïs.
![]()
In rural Africa, solar energy can be up to 50 percent cheaper than using diesel generators. In addition to saving money, replacing diesel, kerosene and wood can also increase up time and reduce indoor pollution. (Photo: Iban Colón/NORCAP)
NORCAP’s five energy experts come from a range of professional backgrounds, from environmental engineering to humanities and entrepreneurship.
“Working with humanitarian energy requires more than technical skills. A sound understanding of end-users' socio-economic context and demographic data, as well as key behavioural competencies like communication, are just a few examples. Women of all backgrounds are needed in this sector", says Rebeca.
The value of good role models and supporting colleagues seems to be a common denominator in the group in inspiring them to choose, and perhaps also to stay, in the field of energy.
"The Accelerator Program is a wonderful platform for knowledge sharing. Coming from very different backgrounds and projects, we can learn so much from each other’s experiences and challenges. My time in the program has only confirmed to me that women have so much unrecognised potential that can change the world", says Nour.
Read the full article here!
